EPIRETINAL MEMBRANE
An epiretinal membrane (ERM) is a layer of scar tissue that forms on the surface of the retina. It arises from a variety of ocular conditions including aging. Over time, an epiretinal membrane can cause the progressive wrinkling of the retinal surface, leading to severe and sometimes irreversible distortion and loss of sight. While surgery can be used to remove the epiretinal membrane and thus stop it from structurally changing the retina, it cannot reverse any severe damage done to the retina. Therefore, vision distorted or lost from the formation of an epiretinal membrane is sometimes impossible to restore. For the most part however, the removal of the epiretinal membrane is sufficient to clear the patient’s vision.
WHAT IS THE DISEASE?
As stated in the introduction, an epiretinal membrane is a layer of scar tissue that forms on the surface of the retina. It can lead to the development of cysts, bumps, or blisters in the retina. An epiretinal layer can arise from aging, an idiopathic disease, trauma, ocular inflammation, diabetes, or retinal detachment. Most often, ERM is predominately caused by aging, making it a widespread disease.
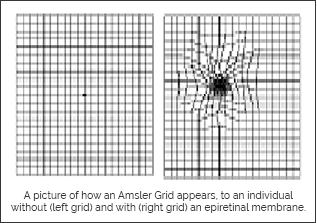
While the underlying cause for the initial formation of the ERM, such as trauma or chronic inflammation, can be stabilized, the ERM can continue to progress and lead to permanent distortion of the retina. It is through the structural alteration of the retina that epiretinal membranes cause severe distortion and loss of sight. Many patients complain of reduce clarity for fine acuity tasks such as reading or distortion of straight lines at a distance. Fortunately, this disease never leads to full blindness.